Revision rhinoplasty is generally considered to be the most complex of all facial plastic and reconstructive problems.
We love to correct problems
PROCEDURES FOR REVISION RHINOPLASTY
VIDEOS




OUR TEAM
We are nationally and internationally known for our expertise in revision rhinoplasty and nasal reconstructions. We therefore serve as a center for revision rhinoplasty (problems caused by previous failed cosmetic and functional rhinoplasty, performed in other clinics/by other surgeons) and nose reconstruction for patients from all over Europe and even beyond.

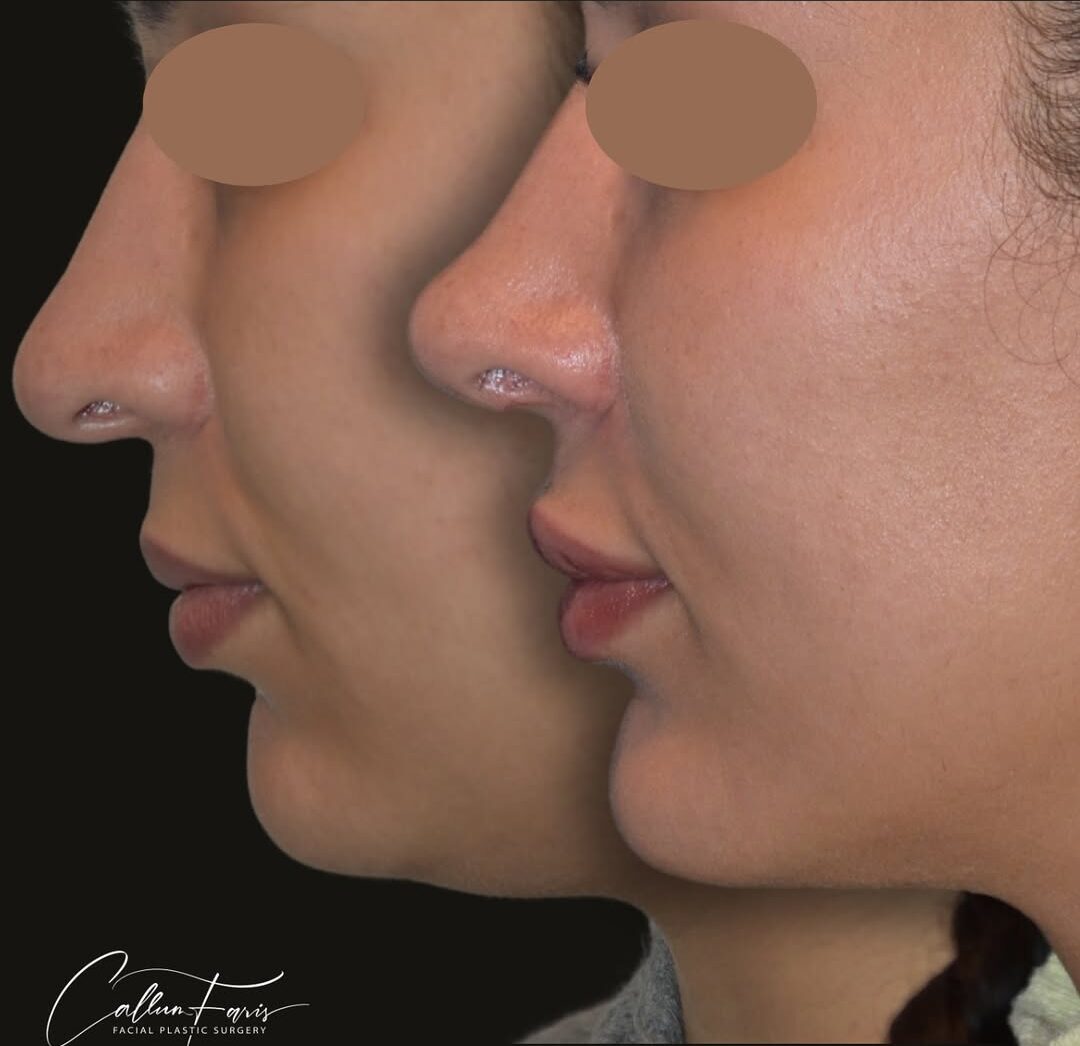
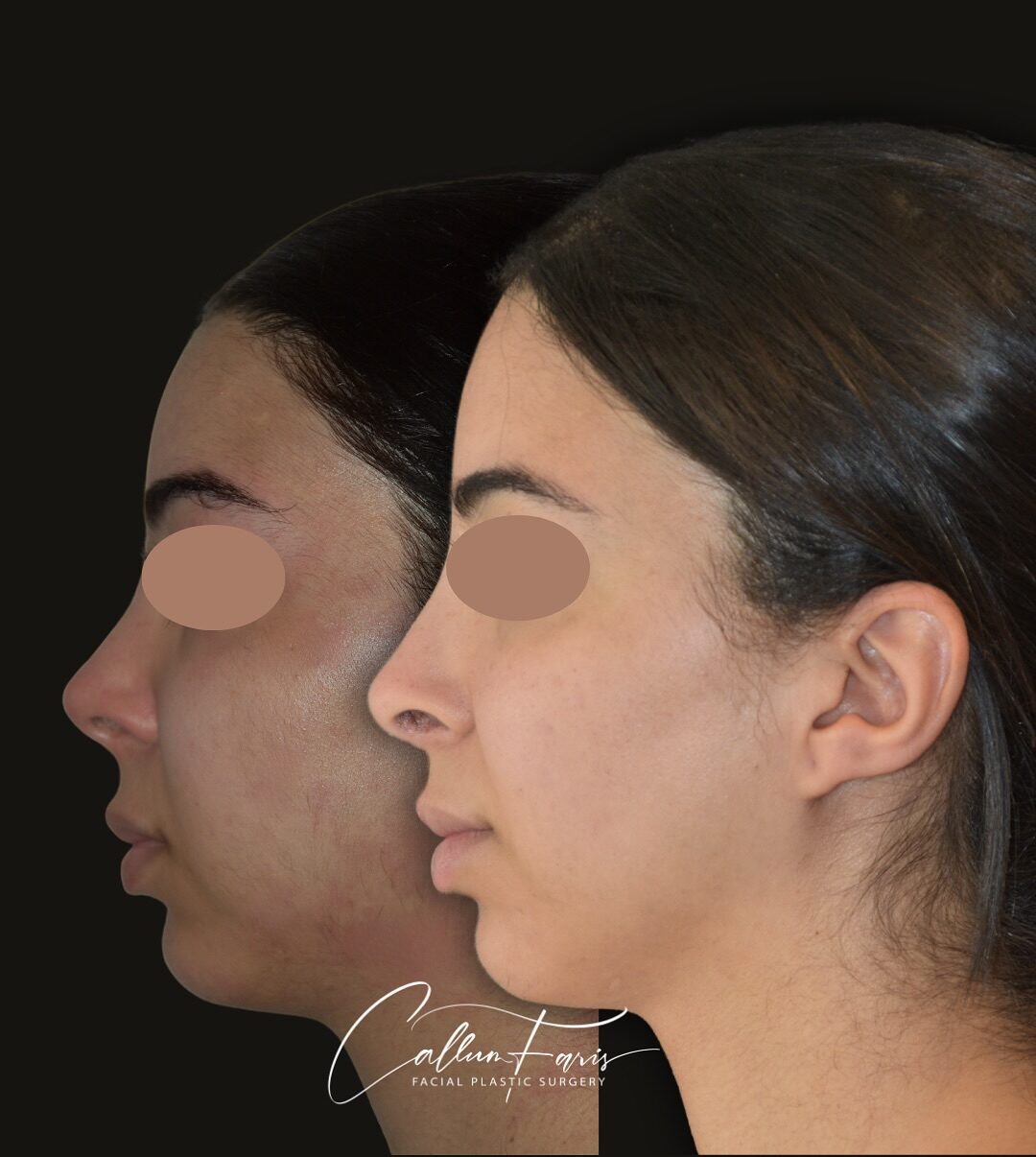
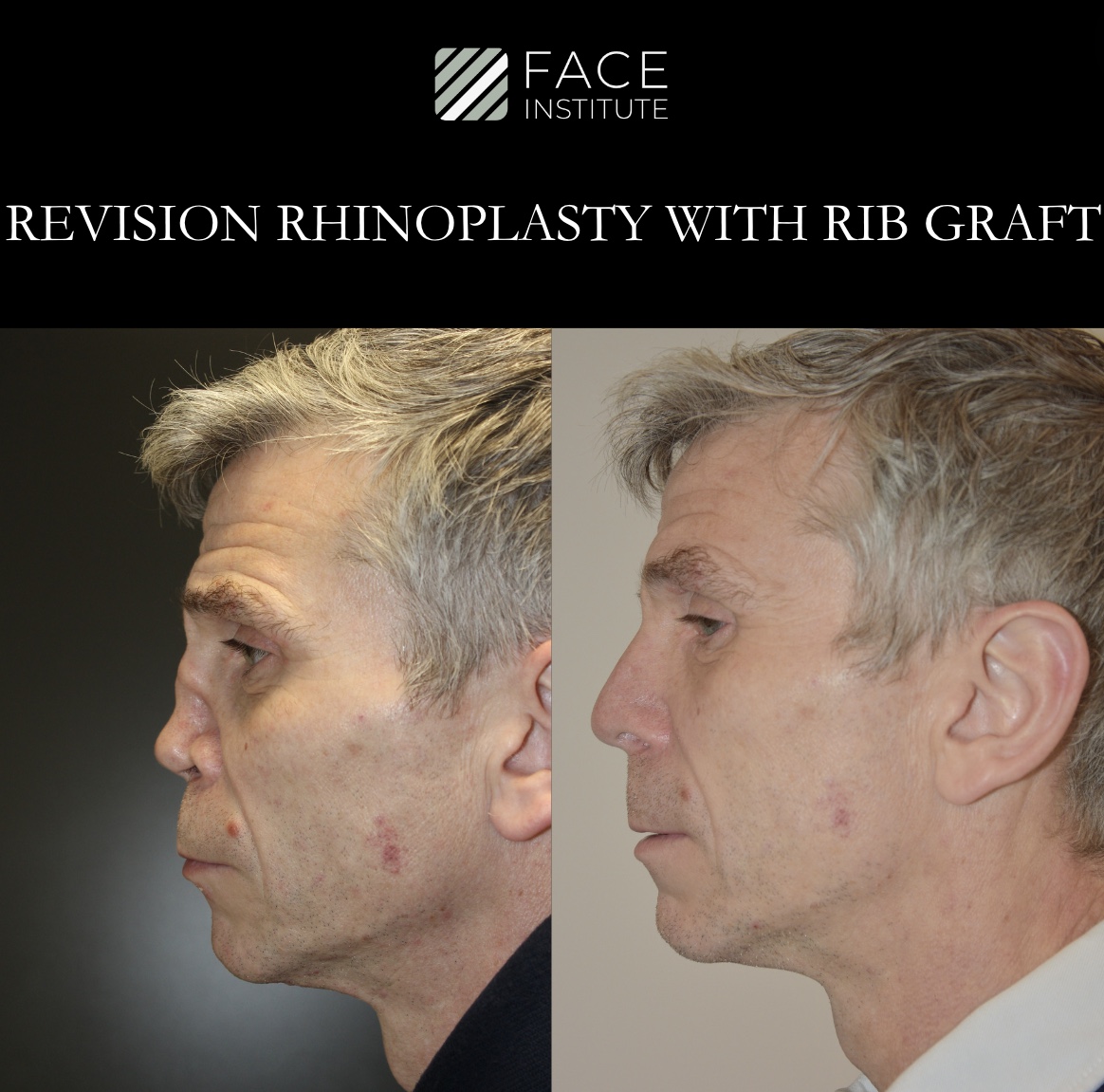
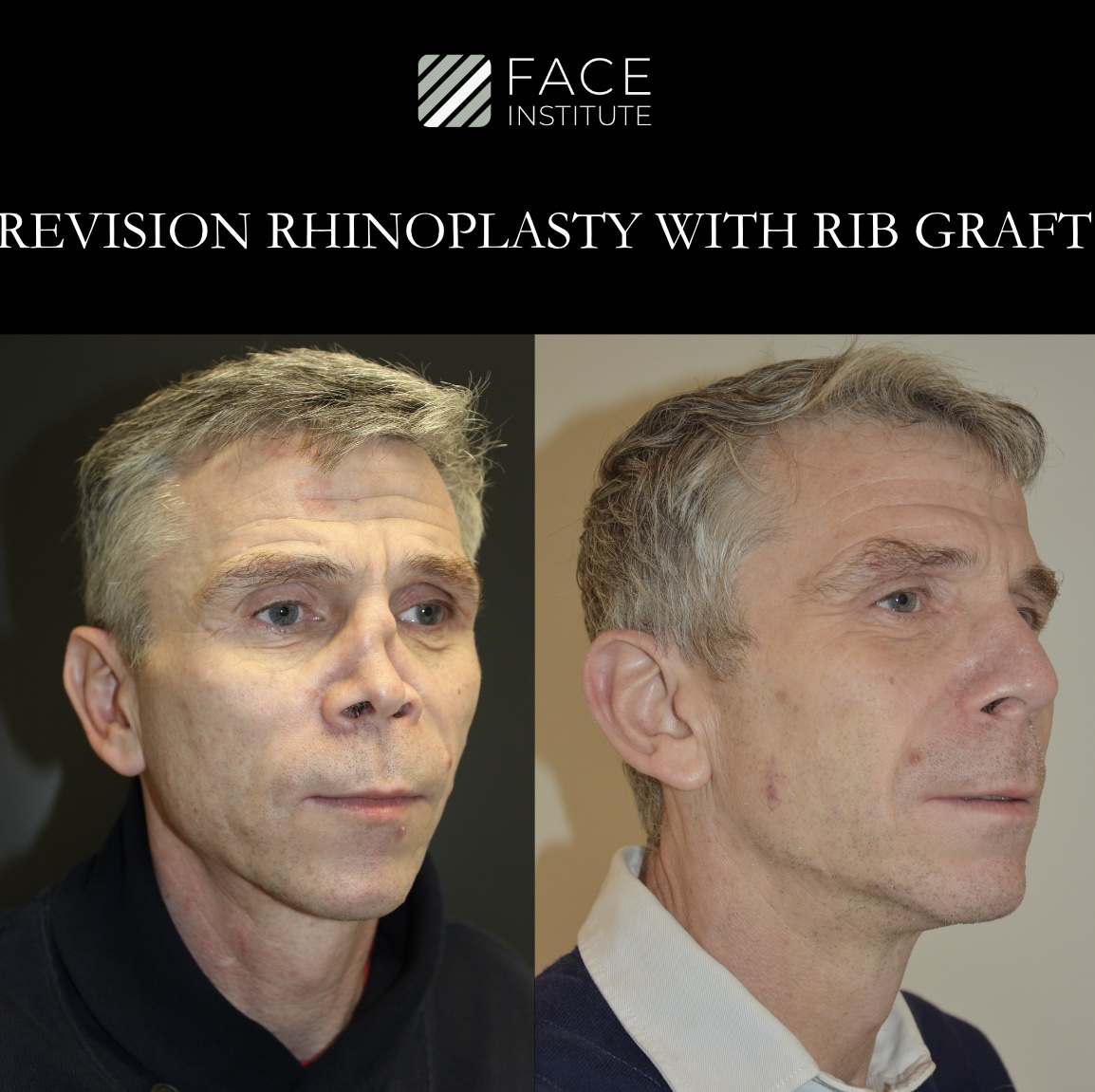
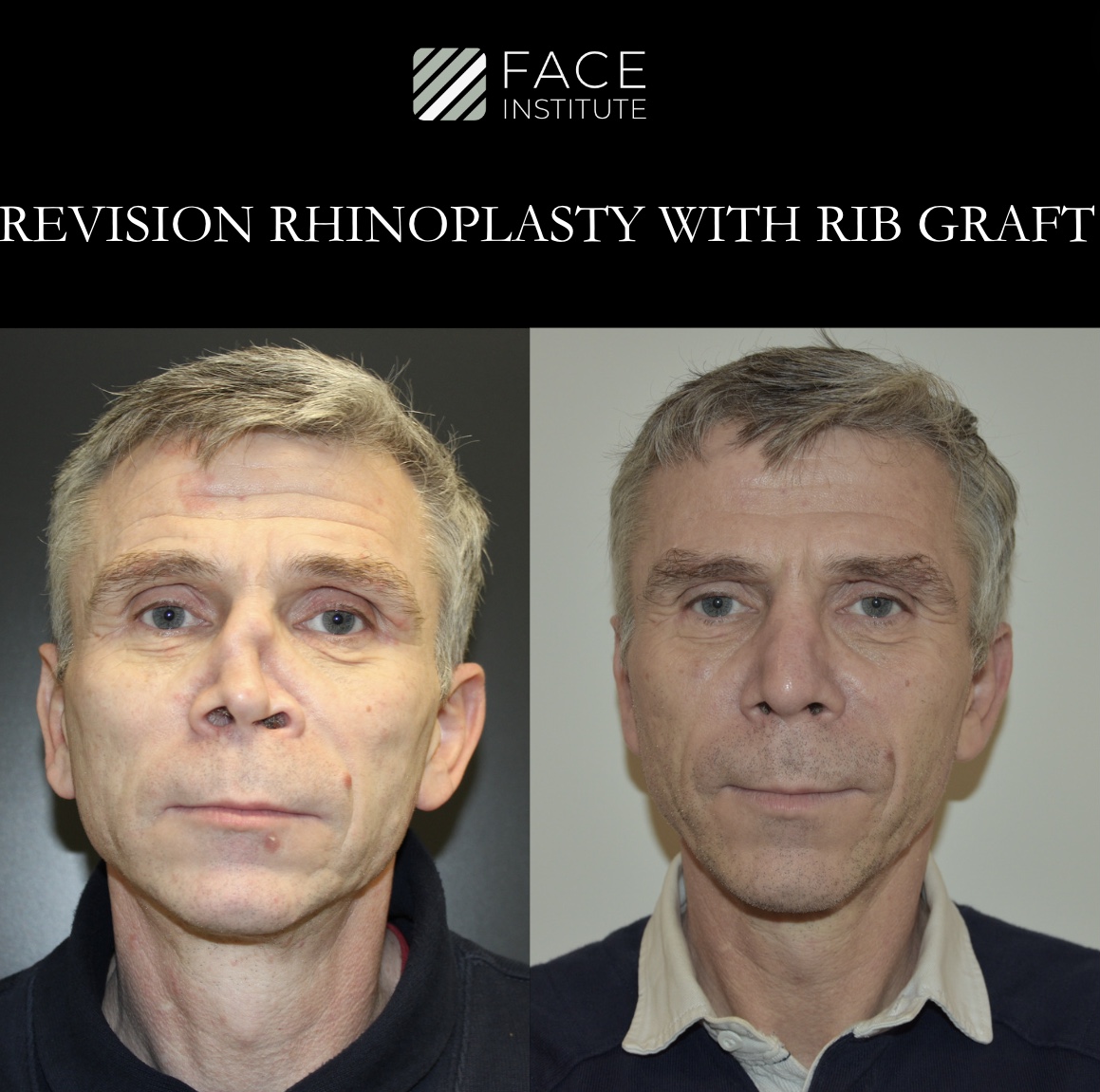
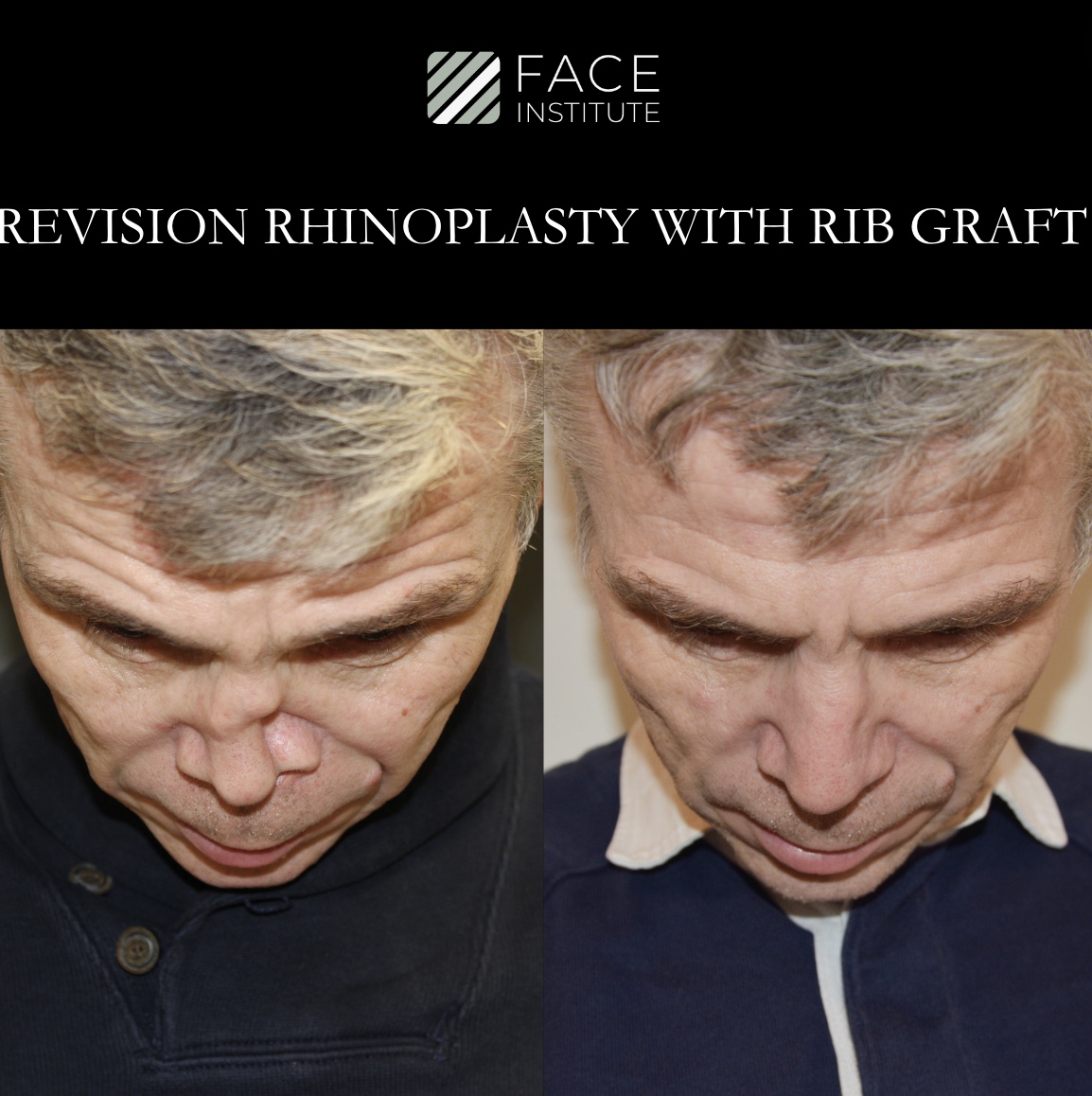
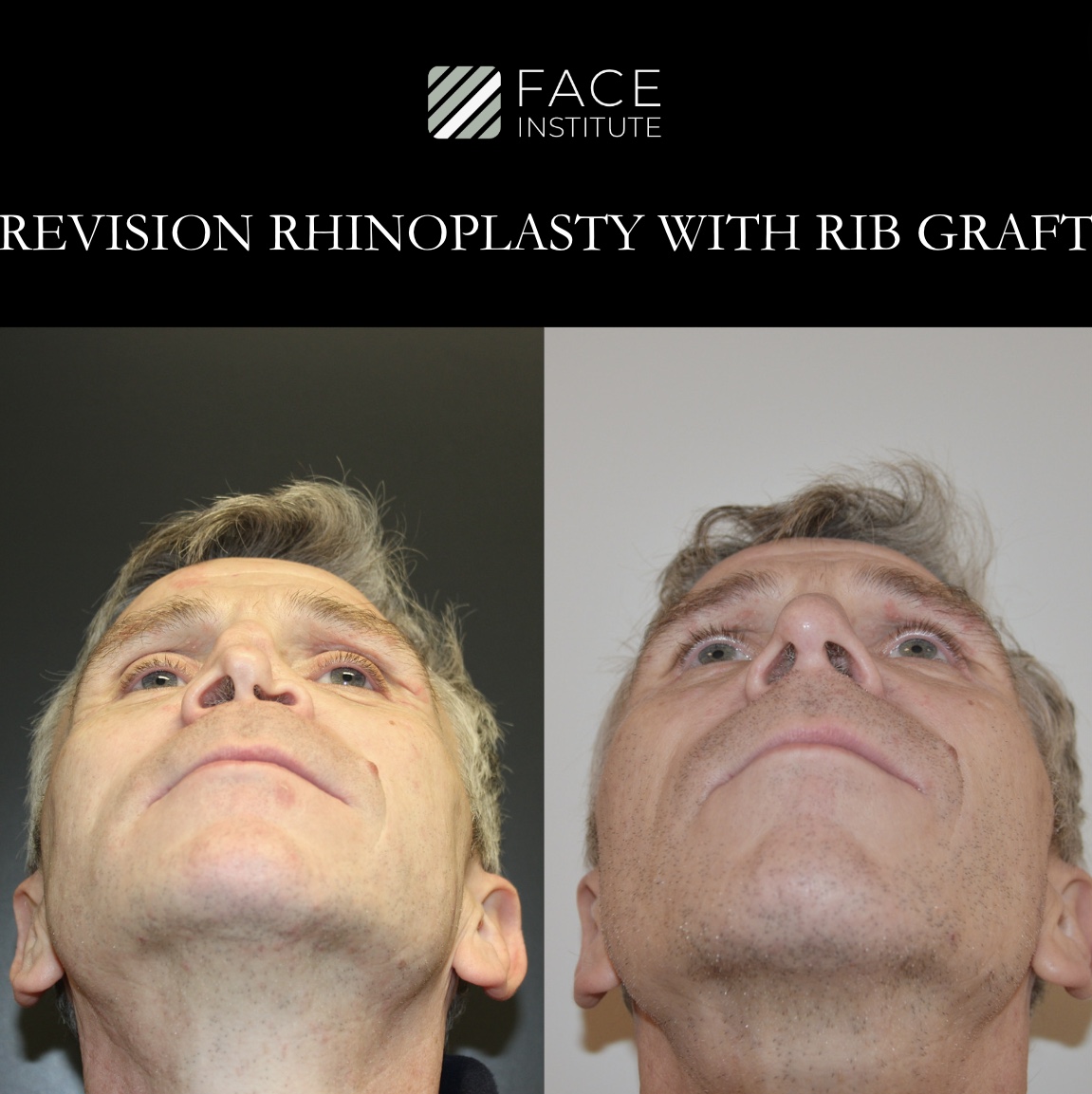
EXAMPLES OF OUR WORK







THE PROBLEMS
Rhinoplasty is a common operation. The results are mainly good to excellent. Unfortunately, we also see a large number of patients in our clinic with problems after undergoing previous operations performed in other clinics or in overseas areas. There are many causes of dissatisfaction, but the most common causes are:
- Breathing problems
- A crooked nose
- A nose bridge that is too low
- Irregularity
- A nose tip turned too far
- A lack of definition of the nasal tip
Our opinion has been asked about almost every problem or complication you can think of as a result of rhinoplasty surgery. As complications become more severe, our approach to the problem shifts from complex revision rhinoplasty to nasal reconstruction. This means that we have a solution for most problems after previous surgery.
What should you do if you are dissatisfied after undergoing a rhinoplasty?
In the event of a rhinoplasty that does not meet the expected results, the first step is to discuss the problem with the relevant doctor. It is especially important to be patient and wait for the nose to heal. Some problems are related to swelling of the tissue and the nose can change over a period of a year. A conversation with your facial plastic surgeon can help you understand whether your symptoms will resolve on their own over time.
If the situation does not improve and you need a second opinion, you can request the details of the operation and the before and after photos from your surgeon. It is common for us to see patients nine months after their original surgery for revision surgery. In the event of an emergency, we will have patients who need urgent treatment come within one to two weeks.
You may be a candidate for secondary rhinoplasty or a revision rhinoplasty procedure if you are unsatisfied after you have healed from surgery. Consult with a facial plastic surgeon who specializes in revision rhinoplasty surgery procedures for a thorough evaluation and potential plan for revision rhinoplasty surgeries. This is important to ensure that you achieve the desired results, and to address any concerns you may have about the surgical procedure.
Anatomical Issues:
1. Persistent nose deviation:
This can be annoying for patients and is often the primary concern for revision rhinoplasty. Some patients with persistent nasal deviation have in fact a degree of facial rotation, roughly 1/3. This means the nose can never be totally straight, but the nasal deviation can usually be improved. This will be explained to you in the consultation with Doctor Faris.
2. Irregularity of nasal dorsum:
Achieving perfect smooth dorsum rhinoplasty is challenging and is one of the major limitations of Structural Rhinoplasty. Due to this fact, we now use new techniques such as Dorsal Preservation Rhinoplasty where the dorsum is preserved and the whole nasal framework is lowered as a unit. This helps create a smooth Dorsum. If you’ve had a previous structural Rhinoplasty, you are most likely not a candidate for Dorsal Preservation Rhinoplasty. However, your dorsum can be made smooth with further rasping and smoothing of the nasal bones and cartilages with Burs and Rasps. Additionally masking the dorsum with crushed cartilage, PRF fascia or rib perichondrium. There are many techniques that we use in the Face Institute, but we will choose the specifically the best technique for your requirements.
3. Lack of facial harmony:
You cannot look at the nose alone in the face. There are aesthetic ideals for face and nose dimensions from the most attractive female faces and different dimensions from the most attractive male faces and noses. However, this does not take into account age, ethnicity, and personal taste. These other factors are of vital importance: the anatomy of your forehead, the anatomy of your chin, and the anatomy of your lips. When you look at the side view in (the profile view), you can see the appearance of the nose can change depending on if the chin is small or large or the forehead is prominent or not. Therefore, you must take into account all of these factors. Failure to do so will result in a lack of harmonization in the face which can be a significant problem after primary rhinoplasty. In some instances, the primary Rhinoplasty was performed without taking into consideration the overall face and therefore the results of optimal having a consultation with us at Face Institute. We will analyze the entire face, your chin, your forehead, your skin quality, skin thickness and also your ethnicity and your aesthetic wishes to help explain to you what are the best options in harmonizing your nose with your face.
4. Over-stylised nose:
Styles come in and out of fashion. One of the problems of having a highly stylised nose is that it may not be the look that you wish to have for the rest of your life.
Remember having a Rhinoplasty is for life (unless you have a revision). We often see patients who have had a highly stylised short nose with an upturned tip and a very rotated tip. See below in the photo. Often these patients have not requested this alteration and the result of surgery is an unwanted, often due to a breakdown of communication in the aesthetic aim for surgery between the previous surgeon and the patient.
These are difficult problems to correct. The nose needs to be made longer. The tip to be de-rotated after the tip is made wider. There are usually other associated defects that have to be corrected, and these cases usually require rib grafting and longer operative times.
5. Nasal Obstruction:
Please see the section below for functional issues:
Over resection of dorsum: Aggressive removal of nasal cartilage or bone can cause structural weakness, leading to a collapsed or pinched appearance. This may affect both aesthetics and functionality.
6. Open roof deformity:
Occurs when the dorsum has a roof that has been opened to reduce the dorsal hump or the height of the dorsum but then the nasal bones have not been fractured inwards, so the exists a gap of tissue over the nasal dorsum. This is called an open roof deformity. It requires revision of the nasal dorsum and in-fracturing of the nasal bones through revision osteotomies.
7. Over resection of tip cartilages- Bossae of the tip.
Alar cartilage gives the shape of the lower third of the nose and also gives the lower third of the nose strength. When cartilages are reduced there are three outcomes.
A. The cartilages are made smaller. The reduction In size is usually an aesthetic advantage and is planned producing a more refined smaller less wide nasal tip.
In attempts to make the most refined nasal tip some surgeons choose to reduce the width of the email cartridges to 3 or 4 mm. This has a high chance of precipitating the collapse of the nasal tip after a few years. The minimum alar width should be 4- 6 mm at the tip and 7 to 8 mm in the alar body.
The weakness of the alar cartilages enables the cartilages to be distorted with healing forces and scar contraction. These cartilages can be drawn upwards with scar retraction forces and they can then buckle and bend. This can creates un-aesthetic twists to the nasal tip which show through the skin as white, regularities of the tip and tip asymmetries – these are called nasal bossae.
B. You create a potential space above the cartilage, where the cartilage has been resected.
In the pre-operated position, the alar cartilage sits within a perfectly sized soft tissue pocket. So using the analogy of a hand and a glove, a size 8 hand fits in a size 8 glove. When you reduce the alar cartridge width, the soft tissue pocket does not reduce. So the result is a size 6 hand in a size 8 glove. So you have created a potential space for the cartilage to move in and allow the tip and the alar wings to retract upwards. This produces a retracted alar which gives you more nostril show becomes more and can also give the impression that the columella is hanging or has sagged. This is often not the case and actually what you are seeing is just more of the columella because the alar cartilages have been drawn upwards (alar retraction).
8. Nostril Asymmetry:
This can occur for a variety of reasons. Sometimes pre-existing abnormalities in the nose congenitally formed. Nasal asymmetry symmetry can also exist from deviation of the caudal septum. It can also occur from asymmetrical alar base reductions – Alarplasty. It can also occur from alar retraction.
It is the end product of a variety of underlying problems such as skin deficiency, webbing, alar cartilage malformation and alar cartilage insufficiency.
Treatment is dependent on the cause and can be challenging to correct. Often only improvement is possible not full correction.
9. Persistent Dorsal hump:
Most females, wanting Rhinoplasty prefer either a small gentle, concave, dorsum or a straight dorsum. Most males, wanting Rhinoplasty prefer either a small residual hump or a straight dorsum. The skin thickness of the dorsum is a variable and therefore this must be taken into consideration when creating the dorsal profile.
Other factors of importance are the factors is that you can have a bone reaction from lowering the nasal bones that can cause osteitis and some small new bone formation and recurrence of a small hump in the post-operative phase. Profile dorsal alignment is one of the most challenging parts of Rhinoplasty. The good news is, however, that small residual dorsal humps are relatively easy to correct, normally with a small revision.
10. Visible cartilage grafts:
InIn the 1980s and 1990s and 2000’s grafting of the nasal tip was commonplace in almost all surgeries, even including primary rhinoplasties. We learnt over time that many of these grafts became visible years after surgery. This is an interplay between graft size and thinning of the tissues with age and also the thickness of the patient’s skin. This was difficult to predict. Due to this we now try to avoid doing tip grafts in primary rhinoplasty unless absolutely necessary. In some instances, grafts are required, but it is the exception rather than the rule.
In revision rhinoplasty grafts are normally needed. So existing grafts are removed or modified or covered with fascia to soften the edges of the tip graphs. If you are having a full revision, normally these graphs are removed and new grafts are fashioned, or the underlying tip cartridges are strengthened to reduce the requirements for tip grafts.
11. Saddle nose deformity
This is where there is collapse of the nasal dorsum, producing a sagging that looks like the curvature of a saddle of a horse. This is due to lack of support from the septum and can be from excessive resection of the cartilage, or from except the perforation. These can be corrected with the reconstructive Rhinoplasty techniques and cartilage crafting from the air or from the rib good outcomes are expected.
Functional Concerns:
12. Breathing Difficulties:
Changes to the internal nasal structures can impact airflow. Patients may experience persistent nasal congestion, snoring, or difficulty breathing through the nose.
These can be either from the septum, a nasal valve problem, lining inflammation or stenosis or web reducing the cross section area of the nasal airway.
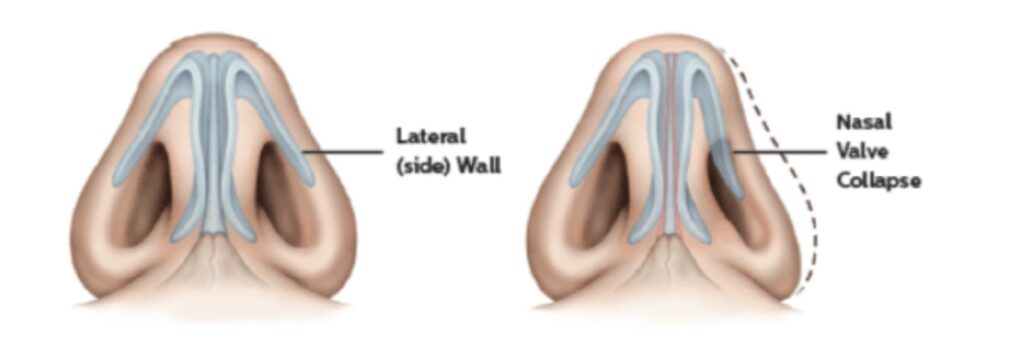
13. Nasal Valve Collapse:
Weakening of the nasal sidewalls, known as the nasal valves, may occur after rhinoplasty. This can result in breathing issues and a narrowed appearance of the nostrils.
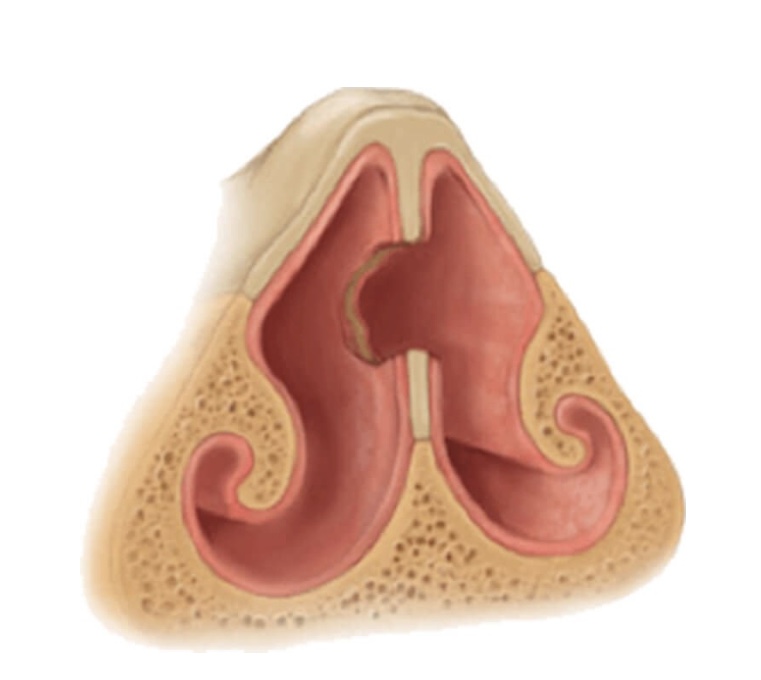
14. Septal Perforation:
An unintended hole in the nasal septum can develop, causing airflow disruption, whistling sounds, and potential long-term complications.
We are a specialist center for perforation repair. We have an international clientele for this, and we have one of the highest rates of successful septal perforation repair published anywhere in the world. We often perform sets for perforation repair in isolation or combined with cosmetic rhinoplasty or combined with a provision, functional and or revision cosmetic Rhinoplasty. To perform such a professional pair with those reconstructions. For perforations under 3 cm we have an over 95% closure rate.
15. Internal scars in the nose
Internal scarring and webbing of incisions can take place. These can limit the airflow in the nose and cause symptomatic nasal obstruction.

Indications for Revision Rhinoplasty
Recognizing the need for revision rhinoplasty involves a combination of patient symptoms and clinical evaluation. Indications may include persistent aesthetic dissatisfaction, ongoing functional problems, or both. Patients need to communicate openly with their surgeon and seek a second opinion if needed.
Conclusion
While many individuals achieve their desired results with rhinoplasty, some may encounter anatomical and functional issues that necessitate revision. Understanding the potential concerns, staying vigilant for symptoms, and maintaining open communication with the surgeon are crucial steps in navigating the post-rhinoplasty journey. Revision rhinoplasty, when performed by a skilled and experienced surgeon, can address these issues and help patients achieve the optimal balance of form and function.
Summary
Revision rhinoplasty poses greater complexity compared to the initial surgery due to prior alterations to the nasal framework. The previous procedure may have depleted nasal cartilage, limiting available material for the revision. Consequently, cartilage grafts from donor sites on the body may be necessary. Moreover, dealing with scar tissue from the primary surgery demands meticulous manipulation to achieve seamless results. Given the intricate nature of revision rhinoplasty, the open approach is often preferred, providing surgeons with enhanced access and visibility, especially when addressing changes to the nasal tip.
Choosing a Revision Rhinoplasty Surgeon; Regardless, akin to primary rhinoplasty, selecting a qualified and experienced facial plastic surgery specialist is paramount to ensure the fulfillment of your aesthetic goals and minimize the likelihood of future revisions.
OUR CLINICAL ASSESSMENT
An in-depth consultation is important to get a good idea of your cosmetic goals. Your face is unique and our surgical plan will be tailored to your needs. We use image editing software to give you an idea of the different options that our operations offer, so that a decision can then be made about the plan of action.
The operation – the latest techniques
Thanks to the use of precise preoperative planning, we can further improve the accuracy of our operations. We regularly use the piezo ultrasonic machine for our rhinoplasties. This minimizes soft tissue damage, bruising and gives us the unparalleled ability to shape nasal bones much more precisely than previously possible. This technique is called “rhino-sculpture” and simply means more precision, fewer complications and faster rehabilitation.
TRANSPLANTS
For transplants, we only use your own tissue in your nose. We use biological transplants that are rich in growth factors from your own tissue. These plants are specially formulated for each patient, to improve the results and recovery time of our patients. This allows us to minimize the risk of infection and tissue damage to <1%.
Revision rhinoplasty: the most complex of all facial plastic and reconstructive problems
Despite the fact that our focus is on rhinoplasty and we maintain a successful surgical practice to date, we, like other rhinoplastic surgeons, are also confronted with disappointing results. Although adverse outcomes are less likely to occur in the hands of a skilled surgeon, technical skill does not always guarantee a positive outcome.
Although most unsatisfactory results can be improved by additional treatments, there may still be patients who are limited by aspects such as insufficient tissue, unfavorable healing properties and/or pre-existing damage to the tissue. A beautiful nose is medically impossible for only a small percentage of people.
EXECUTIVE DOCTOR

CALLUM FARIS
ENT specialist and specialist in facial plastic surgery